Nationally relevant
Articles relevant beyond the local area
Articles relevant beyond the local area

UPDATE: View our video recording of the full 45-minute event at motifri.com/wp-content/uploads/2022/03/Ukraine-vigil.2022-03-26-720p-h264-crf35.mp4 An umbrella group calling itself “Rhode Islanders for Ukraine” announced a vigil in support of the Eastern European nation, now fighting against an invasion by Russia, to be held Saturday, March 26, at 4pm on the south side of the RI State House, […]

As retail gasoline prices rise above $4.00 per gallon, a lot of misinformation and even disinformation is circulating purporting to explain this. Let’s try to get to the real reasons. The historical peak for retail gasoline was in 2008 when the consumer price reached what would be $5.20 per gallon today, adjusted for inflation, and […]

Neo-Nazi protesters waving flags emblazoned with a swastika, “SS” runes, and a “Totenkopf” (death’s head) disrupted an event at Red Ink Community Library on Cypress Street near Billy Taylor Park in Providence. The reading at 6pm on Monday, Feb 21, was intended to commemorate the 174th anniversary of The Communist Manifesto as part of international […]
A federal mandate issued by the Centers for Medicare and Medicaid Services (CMS) requires health insurers to either directly cover or indirectly reimburse each insured individual for up to eight at-home over-the-counter COVID-19 rapid antigen test (RAT) kits per month, up to $12 per test. Families on the same insurance plan are eligible for RAT […]
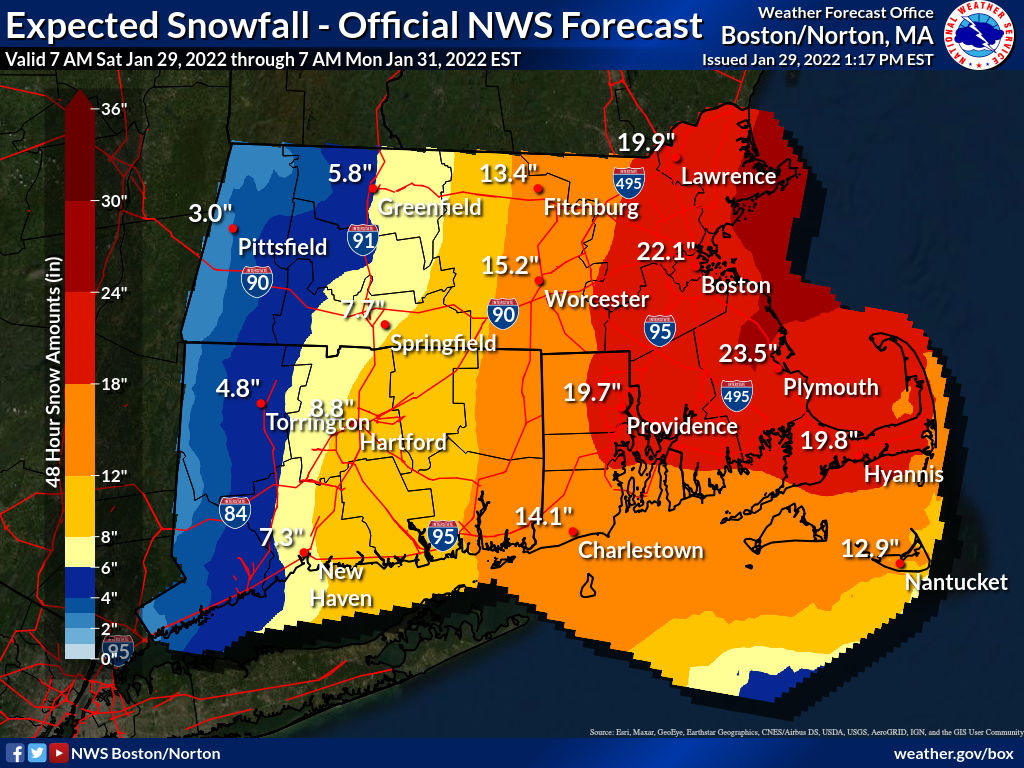
Blizzard Warning in effect from Sat Jan 29, 12:00am EST until Sun Jan 30, 12:00am EST. RI has declared a state of emergency and imposed a travel ban Sat until 11:59pm for all vehicles. RIPTA has suspended all service Sat. A classic “nor’easter” winter storm is bringing blizzard conditions and an estimated 12–24 inches of […]
Every residential address in the US can order four rapid antigen test (RAT) kits for free, expected to be delivered in late January, through an official government web page: covidtests.gov (which currently redirects to a site operated by the US Postal Service special.usps.com/testkits). Persons need enter only their name and shipping address to place a […]

Dr Nicole Alexander-Scott, MD, MPH, who has served as director of the RI Department of Health (RIDOH) since 2015 and spearheaded the state’s response to the COVID-19 pandemic from the beginning, has resigned effective two weeks from today, according to a statement from Gov. Daniel McKee, and the governor “regretfully accepted.” She will continue in […]
At time of writing, RI is in bad shape for COVID-19, with a surge of cases unprecedented over the course of the entire pandemic. RI is weeks behind where it could have been if it had taken into account clear warning signs. At a Woonsocket press conference with Gov. Daniel McKee and others on Dec […]
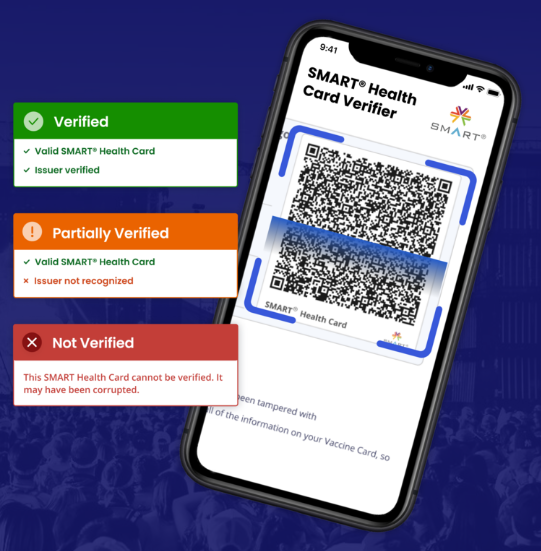

(App download links at end of article.) RI has updated and renamed its “401Health” app (previously “Crush COVID RI”) for Google Android and Apple iOS, the office of Gov. Daniel McKee announced today. The main purpose of the update is to add support for displaying the user’s vaccination record via a securely trusted QR code, […]

Treatment with monoclonal antibodies (MABS) is recommended and authorized to keep patients who test positive for COVID-19 out of the hospital, reducing the severity of mild to moderate symptoms. The treatment is done on an outpatient basis by a one-time infusion that takes several hours. In RI, however, there is a logistical backlog on quickly […]